Bpc 157 Organic Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Introduction: When “multifunctional” becomes a research problem
If you’ve ever tried to make sense of peptides that are marketed as having broad “healing” potential, you know the real pain point: the claims sound unified, but the evidence is scattered across papers, patents, and experimental designs. In my hands-on literature review work, I’ve repeatedly seen the same issue—people jump straight to conclusions about bpc 157 organic activity without separating (1) what’s been observed in specific models, (2) which outcomes are actually mechanistically supported, and (3) how patent language may differ from peer-reviewed results.
This article reviews the multifunctionality theme and potential medical application of BPC 157, focusing on what the literature and patent records collectively suggest—and where they don’t. You’ll get a structured view of the evidence, the biology people commonly connect to these effects, and practical takeaways for how to interpret claims responsibly.
What “multifunctionality” means for BPC 157 in the literature
“Multifunctionality” is a word that gets used when a single compound is linked to multiple physiological outcomes—often including tissue repair, inflammation modulation, and functional recovery across different organ systems. For BPC 157, the multifunctionality narrative usually comes from a pattern: studies report beneficial endpoints in distinct injury contexts, frequently in preclinical settings.
How I evaluate multifunctionality claims
In my own review workflow, I look for four things before treating multifunctionality as more than a marketing concept:
- Outcome specificity: Are the endpoints clearly defined (e.g., measurable healing markers, functional scores) or are they only descriptive?
- Model comparability: Are studies using comparable injury severity, dosing schedules, and assessment timing?
- Reproducibility signals: Do independent studies using similar experimental designs show consistent directionality?
- Mechanistic plausibility: Is there a coherent mechanistic thread (even if incomplete), rather than isolated “it worked” observations?
Common multifunctionality themes
Across the literature and patent disclosures, BPC 157 is often discussed in relation to:
- Gastrointestinal and mucosal repair endpoints (where BPC 157 is frequently discussed)
- Tissue repair and recovery after localized injury
- Inflammation-related signaling changes
- Organ-protective effects framed around functional restoration
The key logic behind the multifunctionality framing is that some biological pathways—such as those governing epithelial repair, inflammatory response, and tissue remodeling—can appear across multiple injury models. Still, “cross-model effects” does not automatically mean “one unified mechanism,” and that distinction matters when you translate research into real medical application expectations.
BPC 157 and potential medical applications: where the alignment is strongest
When people ask about possible medical application, they’re usually asking two questions: “What conditions have been targeted?” and “What level of evidence exists for each?” In reviews like the one reflected by the title you provided, the safest approach is to map applications to evidence strength by category.
1) Gastrointestinal injury and mucosal protection
In many accounts, the gastrointestinal tract is the best-established thematic home for BPC 157. The rationale is straightforward: if an intervention reliably improves mucosal integrity or recovery in relevant experimental injuries, it becomes a candidate for application areas such as:
- mucosal injury contexts
- models of impaired barrier function
- recovery after chemically induced or stress-related insults (as described in preclinical literature)
Why this matters: For medical translation, endpoints that relate to barrier function and measurable healing signals are often easier to standardize than broader claims like “general healing.”
2) Soft tissue and repair-focused contexts
Another frequent application direction is tissue repair after injury—particularly where restoration of structural integrity and recovery of function are measured.
Practical lesson from reviews: I’ve found that when papers report improvement in “repair,” you still need to check whether they’re measuring structural outcomes (histology, cellular markers) versus purely functional readouts. A treatment may improve one but not the other depending on the model design.
3) Inflammation and downstream signaling endpoints
BPC 157 is also discussed in ways that connect it to inflammation modulation. The underlying logic here is that inflammation is a common upstream driver of impaired healing across many injuries. However, “anti-inflammatory effects” can be a broad umbrella—so the most credible application arguments describe specific signaling changes, receptor/pathway involvement, or consistent biomarker patterns.
Where evidence translation commonly breaks
In my experience reviewing claim-to-evidence chains, the largest translation gaps often show up in:
- Dose translation: Preclinical dosing regimens don’t map neatly to human schedules.
- Administration route: Delivery method can strongly influence exposure and effect profiles.
- Outcome harmonization: Studies may use different endpoints, making “multifunctionality” appear more uniform than it is.
Patent language vs. peer-reviewed evidence: how to interpret both
Patents and academic papers can tell different kinds of truths. Patents often emphasize use claims, compositions, and therapeutic intent; academic literature emphasizes experimental design and reporting. When you review both, you get a fuller picture of how the field frames medical application—even if the legal framing can be broader than the experimental evidence.
What patents typically add
- Scope of claimed indications: Patents may cover a wider set of conditions than any single study tested.
- Formulations and administration details: Legal documents can provide specific dosing/route concepts that aren’t always emphasized in papers.
- Mechanistic framing: Even when mechanisms are uncertain, patents may propose pathway relationships to support utility.
What patents typically cannot replace
- Independent confirmation: A claimed effect still needs replicated experimental validation.
- Clinical outcome evidence: The most relevant “medical application” standard is clinical data; patents alone don’t establish clinical efficacy.
- Risk/benefit clarity: Safety, adverse event profiles, and tolerability are essential for clinical plausibility.
My recommended “two-track” reading strategy
When I combine literature and patent review work, I use a two-track interpretation:
- Track A (evidence): Extract endpoints, timepoints, and model specifics from papers.
- Track B (intent): Extract claimed indications, formulation concepts, and therapeutic framing from patents.
Then I look for overlap: the strongest “possible medical application” arguments tend to be where patent claims align with repeatedly reported experimental outcomes.
About “bpc 157 organic” wording: why terminology matters
Your core keyword—bpc 157 organic—highlights a practical issue I often see: consumers and even some content producers conflate sourcing/labeling terms with biological or clinical meaning. “Organic” is not, by itself, a mechanistic descriptor for peptide activity. What matters is:
- Identity and purity: Confirmed peptide composition and purity can influence consistency of biological results.
- Manufacturing characterization: How batch consistency and analytical testing are handled.
- Stability and handling: Peptides can be sensitive; stability affects what biological system actually sees.
When you see broad claims tied to “organic” labeling, treat them as sourcing descriptors unless the content provides concrete quality-control details tied to biological endpoints.
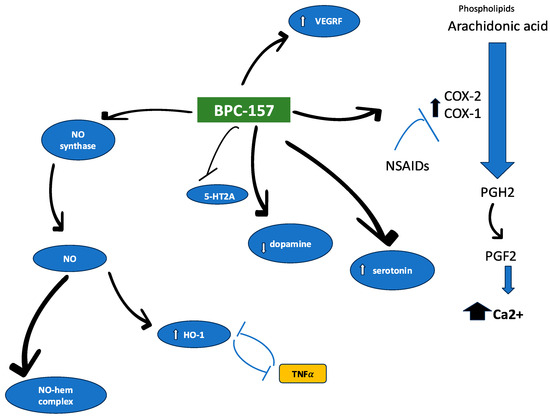
Visual reference: peptide-associated literature figure
What a “best-fit” medical application roadmap looks like
If your goal is to translate multifunctionality claims into a credible application roadmap, the strongest structure is one that moves from standardized preclinical endpoints to human-relevant studies.
Step-by-step roadmap (evidence-first)
- Define target indication precisely: Choose a narrow clinical framing aligned with the strongest preclinical endpoint cluster (e.g., mucosal repair models).
- Standardize dosing and exposure concepts: Ensure studies compare like-for-like where possible (dose, timing, route).
- Prioritize measurable endpoints: Use biomarkers or functional readouts that are likely to translate.
- Clarify mechanism hypotheses: Even partial mechanistic alignment improves interpretability.
- Assess safety signals early: Any candidate medical application must include tolerability and adverse event considerations.
Limitations to keep in mind
Multifunctionality narratives can be compelling, but they can also mask heterogeneity. In the real world, treatments that appear to “help everything” in varied models may have context-dependent effects rather than a single universal therapeutic action.
FAQ
Is “bpc 157 organic” the same as having proven medical efficacy?
No. “Organic” language typically refers to sourcing or labeling, while medical efficacy requires consistent evidence from well-designed experimental studies and, ideally, clinical trials. Terminology does not replace endpoint data.
How should I weigh patents when deciding what medical applications are plausible?
Use patents to understand therapeutic intent, claimed indications, and formulation concepts, but prioritize peer-reviewed evidence for the actual experimental support. The strongest cases are where patent claims overlap with repeated, well-described preclinical outcomes.
What does “multifunctionality” tell us—and what it doesn’t?
It tells you that a compound is associated with beneficial outcomes across multiple contexts. It does not, by itself, prove a unified mechanism, consistent efficacy across models, or clinical effectiveness in humans.
Conclusion: Turn broad claims into a testable application thesis
Multifunctionality and possible medical application of BPC 157 are best understood by separating evidence from framing: preclinical studies suggest multiple beneficial endpoint categories, while patents extend therapeutic intent and use claims. The most credible interpretation happens when “bpc 157 organic” terminology is treated as a sourcing descriptor—not as a substitute for identity, purity, exposure, and measurable outcomes.
Next practical step: Build a one-page evidence matrix for your target indication—list the specific endpoints, model types, dosing/route details, and timepoints from the key papers you find, then check whether the closest patent disclosures claim overlapping use patterns. This creates a clear, evidence-first case for what to pursue and what to doubt.
Discussion